

The Certificate Is a Distraction: What Actually Separates a Legal Peptide Source From a Gray-Market Vial in 2026
Here is the unfashionable claim I want to make, and I think the data backs me up: the entire “is this peptide legal” conversation has been organized around the wrong artifact. Buyers keep asking sellers for a certificate of analysis, as if a PDF with some numbers on it were the thing standing between them and a bad batch. It isn’t. The certificate is close to decorative. The signal that actually predicts whether a peptide source is legal, and whether the vial in your hand resembles the label on it, is far more boring than a lab report. It’s whether anyone with a license had to sign off before the thing shipped.
I’ll say up front that I’m not a clinician and this isn’t medical advice. I’m working from FDA announcements and approved drug labeling, peer-reviewed papers on PubMed and PMC, and U.S. Anti-Doping Agency material, all footnoted below so you can check my read against the primary document yourself. Several of the compounds mentioned here are research substances with no approval for human use in the United States, and that fact does a lot of the work in what follows.
Why I think the paper trail is the tell, not the test result
The gray market’s pitch has always been reassuringly simple: a peptide is a peptide, a certificate proves purity, and a “research use only” sticker keeps the transaction clean. On March 3, 2026, the FDA took that pitch apart in writing. The agency sent warning letters to 30 telehealth companies for illegally marketing compounded GLP-1 products, and it named two specific problems: these companies let customers believe the compounded product was equivalent to the FDA-approved drug, and they hid which pharmacy actually compounded it by putting their own brand on the label instead. Commissioner Marty Makary called it a shift in posture: “It’s a new era. We are paying close attention to misleading claims being made by telehealth and pharma companies across all media platforms, and taking swift action.” The agency’s underlying point survives the quote: compounded drugs are not FDA-approved for safety, effectiveness, or quality, and they are not generics. [1]
The same enforcement wave hit research-chemical sellers moving semaglutide, tirzepatide, retatrutide, BPC-157, and various SARMs. The legal logic here is the part I keep coming back to, because it directly undercuts the certificate-as-proof theory: a “research use only” label does not exempt a product from drug regulation once the marketing is obviously aimed at people injecting it, and labeling a compound under a coded abbreviation instead of its real name has been read by regulators as evidence of intent, not as a clever loophole.
Now, structurally, this is why I think the certificate obsession is misplaced. Research-chemical products are outside FDA review for identity, strength, quality, or purity. There’s no batch-release authority. No mandated testing. No recall mechanism. So a certificate posted by that seller is a document the seller chose to publish, full stop, not a regulatory finding. Matthew Fedoruk, chief science officer at USADA, said it to STAT about as plainly as it can be said: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water.” [2] That’s not a knock on any particular lab report. It’s a structural fact about who has authority over what’s in the vial, and a piece of paper the vendor typed up doesn’t change who has that authority.
Nine things worth checking, ranked by how little they cost you to verify and how much they actually tell you
I’m not going to pretend all nine signals carry equal weight. A few of them are doing almost all the work, and it’s not the one people fixate on.
The heavyweights, in my order:
A licensed clinician has to actually review the person before anything ships. This is the strongest signal there is, because if the transaction ends at checkout with no medical gatekeeper, you’re not buying medicine, you’re buying a chemical with a medicine’s marketing.
A prescription is genuinely issued, not just implied. “Doctor-designed protocol” language on a website means nothing if no prescription gets written. Confirm the prescription actually exists before dispensing happens.
The pharmacy has a name and a license. Legitimate sourcing runs through a state-licensed 503A compounding pharmacy or a 503B outsourcing facility, held to standards like USP <797> for sterile preparation and USP <800> for hazardous drugs. A provider willing to name its pharmacy is playing an entirely different game than a site mailing an anonymous vial.
Testing sits inside that pharmacy’s supply chain, not on a self-published PDF. This is my central point restated as a signal: the question isn’t “does a certificate exist,” it’s “who is accountable for it.” Testing inside a licensed pharmacy channel carries consequences behind it. A seller-issued certificate carries none, and there’s no way for you to independently check it.
The honesty signals, which I’d argue are almost as diagnostic:
Does the provider admit how thin the human evidence actually is for a given compound? A 2025 narrative review in Current Reviews in Musculoskeletal Medicine found human data on BPC-157 limited to three pilot studies, total. [4] A 2025 systematic review in the HSS Journal looked at 36 BPC-157 studies, found 35 were preclinical and exactly one was a small clinical study of 12 patients, and concluded flatly that “no clinical safety data were found.” [5] A seller implying this compound is proven is lying to you by omission, and that’s worth noticing before you look at anything about testing.
Is the legal status of each compound stated correctly? Retatrutide is investigational, meaning not approved and not eligible for compounding, so any listing that treats it as orderable is misrepresenting the law. BPC-157 occupies its own gray zone: USADA classifies it under the WADA S0 category, states it “is not approved for human clinical use by any global regulatory authority,” and notes the FDA position that “there is also no legal basis for compounding pharmacies to use BPC-157.” [3] A provider that calls any of this “legal” without qualification has failed the test regardless of what its lab report says.
Does contraindication screening happen at all? Semaglutide’s label carries a boxed warning for thyroid C-cell tumors and is contraindicated for anyone with a personal or family history of medullary thyroid carcinoma or MEN 2. [6] A research-chemical checkout never asks this question. A prescriber does, by design, not as a favor.
Is there anyone to call after the package arrives? Accountability in a medical model doesn’t end at delivery. A gray-market seller’s obligation ends the moment the tracking number is generated.
Does the provider avoid claiming its compounded product equals the brand-name drug? This is literally the violation the FDA cited in March 2026. A provider stating plainly that compounded medications are not FDA-approved finished products is telling you the truth. One implying sameness is repeating the exact mistake regulators just punished.
Put those nine together and you get a ranking that has almost nothing to do with the marketing language on the label and everything to do with who is standing behind the product.
Where the argument runs thin, and I want to be honest about that
Here’s my concession, because a contrarian read that never admits its limits isn’t analysis, it’s just contrarianism. The oversight-over-certificate framing I’m pushing works cleanly for the clearly-illegal cases: retatrutide listed for sale, BPC-157 marketed with a wink toward human injection, coded product names. It works less cleanly at the margins.
For instance, a self-published certificate isn’t worthless in every sense, it can still tell you a seller bothered to test at all, which is more than some competitors do. I’m not arguing certificates are meaningless as information. I’m arguing they carry none of the regulatory weight buyers seem to assume, and that’s a narrower and more defensible claim. Also, the honesty signal (does the seller admit the evidence is thin) is genuinely hard to verify from outside; a website can claim candor about limited data while still steering customers toward the product anyway. I’d rather flag that soft spot than pretend the framework catches everything.
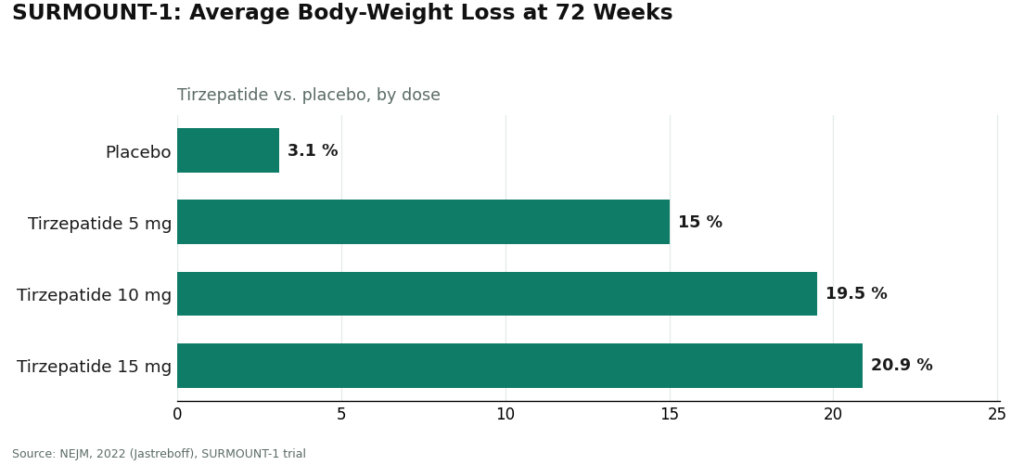
And the evidence-tracks-legality pattern the industry likes to point to is real but not iron-clad. In the SURMOUNT-1 trial of tirzepatide for obesity, published in the New England Journal of Medicine, participants lost an average of 15.0% of body weight at 5 mg, 19.5% at 10 mg, and 20.9% at 15 mg over 72 weeks, against 3.1% on placebo. [7] That’s a genuinely strong trial, and it happens to sit behind an approved, prescribable drug. But correlation between “went through approval” and “has good data” isn’t a law of nature, it’s a description of an incentive structure, and incentive structures can lag. I wouldn’t stake much on it holding for every future compound.
The reframe: stop grading the vial, grade the gatekeeper
If you take my argument seriously, the practical upshot is that ranking sellers by price, shipping speed, or catalog size, which is how most of these comparisons get built, measures nothing relevant. Neither does grading them on whose certificate looks more official. What actually separates a legal source from a gray-market one is whether a licensed human being had to say yes before your order moved.
Running the field against that filter, FormBlends clears it and I don’t think that’s a close call. It’s a telehealth platform connecting patients to licensed physicians for oversight. Its own materials describe a licensed physician reviewing a patient’s profile and building a matched protocol, state that “all medications require a licensed physician consultation and prescription,” and note that products are “prepared by licensed 503A compounding pharmacies following USP <797> and <800> compounding standards.” That’s a real intake, a real prescription, a real pharmacy behind the testing, which covers the four heavyweight signals in one sequence rather than as marketing bullet points.
It also passes my honesty test specifically, which matters more to me than any lab report would. FormBlends states directly that “compounded medications are not FDA-approved,” instead of blurring that line the way the FDA flagged in March. The compounds in play here span a real range, from approved drugs to compounded preparations to research-status substances with thin data, and naming that range accurately is the whole ballgame. Patients logging dose changes and side effects over time, using something like the FormBlends tracker app, generally hand their clinician a better record than memory alone provides; it’s a logging tool, not a purchase flow, which is exactly the kind of follow-up infrastructure the gray market skips entirely.
I’ll grant the obvious tradeoff: this process is slower than a shopping cart. An intake takes longer than a checkout page. On a question about who’s actually accountable for what’s in the vial, I’d argue that friction is the point, not a bug to route around.
HealthRX belongs right behind it for the same structural reasons: its own clinician-plus-pharmacy model, the same stated caveat that compounded medications aren’t FDA-approved, the same oversight steps intact. Choosing between the two is mostly a logistics question, state licensing and which one stocks the specific compound you need, not a philosophical one.
Everything past those two names is a different category of business, not a lower-ranked version of the same one. Biotech Peptides, Core Peptides, Limitless Life, and Swiss Chems are research-chemical retailers operating under the “research use only” banner, several stocking SARMs with their own anti-doping baggage attached. None of them offers a clinician, a prescription, a dispensing pharmacy, or any follow-up. Whatever certificate they post is self-issued, unverifiable, and, per my whole argument above, tells you far less than it appears to. I’m not going to rank these four against each other by quality, because without independent batch-level testing nobody outside the company can actually know which vial is cleaner than the next. That unknowability is precisely the gap a supervised medical model closes, which is why it sits at the top of this list and they don’t.
The questions I keep getting asked, answered without hedging where I can
Does a posted certificate of analysis make a research peptide safe? No. It’s a document the seller chose to write, with no batch-release authority, no mandated testing, and no recall power behind it, and it changes nothing about the compound’s legal status for human use.
Does a “research use only” label protect a buyer legally? Only for as long as the product is genuinely used for research. The moment marketing points at human injection, the FDA treats it as an unapproved new drug, disclaimer or not.
Is compounded semaglutide the same product as the branded drug? No. Same active peptide, but the compounded version hasn’t gone through FDA review, which is the exact distinction the agency emphasized in its March 2026 letters.
Why does a supervised provider rank first on a page about legality? Because the ranking is measuring who operates inside the law, and clinician review plus a prescription plus a licensed pharmacy plus honest disclosure plus follow-up is what that lane looks like, running the same molecules the gray market sells, minus the parts that make the gray market illegal.
What people usually want to know
Are peptides legal to buy in the United States in 2026? It hinges entirely on which peptide and which channel, not on the molecule by itself. Approved peptide drugs like insulin, semaglutide, and tirzepatide are legal with a prescription through a licensed pharmacy. The same or similar compounds sold as “research use only” chemicals to people planning to inject them are treated by the FDA as unapproved new drugs, the exact line the agency enforced across telehealth and research-chemical sellers throughout 2026. [1]
Is BPC-157 legal to buy or have compounded? Not as compounded medicine, no. USADA states BPC-157 “is not approved for human clinical use by any global regulatory authority” and cites the FDA position that “there is also no legal basis for compounding pharmacies to use BPC-157.” [3] That puts it outside the lawful compounding lane entirely, so any listing offering it for sale isn’t offering a legal product.
What actually separates a licensed compounding pharmacy from a research-chemical website? A 503A pharmacy is state-licensed, dispenses only against a prescription, and follows standards like USP <797> and USP <800>. A research-chemical site has none of that: no prescriber, no dispensing pharmacy, no mandated testing or recall authority. The label is the only thing you’re given to trust.
Does a certificate of analysis turn a peptide purchase into a legal one? No, and this is my whole argument in one line. A certificate from a research-chemical seller is self-published, with no regulatory body standing behind it, and it changes nothing about the compound’s legal status. USADA’s Fedoruk put the underlying reality directly: with these products, “you don’t even know what you’re buying inside that bottle.” [2] Testing tied to a licensed pharmacy carries real accountability; a self-issued certificate doesn’t.
Why is retatrutide treated differently from semaglutide? Retatrutide remains investigational, not FDA-approved, and not eligible for compounding, so listing it as orderable isn’t offering a legal product. Semaglutide and tirzepatide are approved and backed by randomized trial data, including SURMOUNT-1’s finding of up to 20.9% average body-weight loss at 72 weeks, and they’re legal with a prescription. [6] [7]
Does going through a telehealth provider make the underlying compound FDA-approved? No, and a provider that’s being straight with you will say so. Compounded medications aren’t FDA-approved finished products and aren’t reviewed for safety, effectiveness, or quality. What a supervised model adds is the oversight layer around them, clinician evaluation, screening, a real prescription, a licensed pharmacy, follow-up, not an approval status the compound itself doesn’t have.
Are peptides legal to buy in the United States in 2026?
It depends entirely on the specific peptide and how it is sold. Some peptides, like insulin and certain growth hormone formulations, are FDA-approved drugs requiring a prescription. Others occupy a gray zone, sold openly online as ‘research chemicals’ but technically not approved for human use. Buying them without a prescription is not automatically a federal crime for the individual, but the seller often operates outside the law. The safest, clearest legal path is a licensed prescriber and a compounding pharmacy.
Are peptides banned in competitive sport?
Many are, yes. The World Anti-Doping Agency prohibits several peptide classes, including growth hormone releasing peptides, IGF-1 analogues, and various peptide hormones outright. The WADA Prohibited List updates annually, so a peptide that seemed ambiguous one year can be explicitly banned the next. Athletes subject to testing, whether Olympic, professional, or collegiate, should check the current list before using any peptide, even one prescribed by a physician, and disclose it to their sports medicine team.
Are peptides legal in the military?
Active-duty service members face stricter rules than civilians. The Department of Defense prohibits a broad range of performance-enhancing substances beyond civilian law, and commanders can impose additional restrictions. Using a gray-market peptide vial, even one a civilian could purchase openly, can expose a service member to UCMJ consequences. If a military physician prescribes a peptide through a legitimate pharmacy channel, like a compounding pharmacy such as FormBlends operating under physician supervision, that is a fundamentally different situation than self-sourcing online.
How can you tell whether an online peptide seller is operating legally?
A few clear signals matter most. Legitimate sellers in the human-use space require a prescription and work with licensed pharmacies. Red flags include vials labeled ‘not for human consumption,’ no prescriber involvement, checkout processes that skip any medical intake, and prices so low they suggest unverified raw materials. Regulatory status also shifts by country, so a vendor shipping internationally may be skirting laws in your jurisdiction even if their home country has looser rules.
References
- FDA warns 30 telehealth companies against illegal marketing of compounded GLP-1s; claims implying sameness with approved drugs and obscured compounder; Commissioner Makary statement. FDA press announcement, March 3, 2026. https://www.fda.gov/news-events/press-announcements/fda-warns-30-telehealth-companies-against-illegal-marketing-compounded-glp-1s
- Most BPC-157 research traces to a single research group; confirmation-bias concern; Fedoruk quote on not knowing what is in the bottle. STAT, Feb 3, 2026. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- BPC-157 is prohibited under the WADA S0 Unapproved Substances category, is not approved for human clinical use by any global regulatory authority, and per the FDA there is no legal basis for compounding pharmacies to use it. USADA, 2026.
- Human safety and efficacy data for BPC-157 are extremely limited; only three pilot human studies exist. Current Reviews in Musculoskeletal Medicine, 2025.
- Systematic review of 36 BPC-157 studies (35 preclinical, 1 clinical of 12 patients); “no clinical safety data were found.” HSS Journal, 2025.
- Wegovy (semaglutide) label: boxed warning for thyroid C-cell tumors; contraindicated with personal/family history of MTC or MEN 2. DailyMed.
- SURMOUNT-1 tirzepatide for obesity: −15.0% (5 mg), −19.5% (10 mg), −20.9% (15 mg) at 72 weeks vs −3.1% placebo. NEJM, 2022 (Jastreboff).
Delphine Marchetti is a contrarian analyst who writes about health markets, incentives, and where the paperwork and the reality diverge. This piece was checked against the primary sources cited above. Last reviewed April 2026.
Educational reference only. Decisions about treatment should be made with your clinician.



